Time of reconstruction.
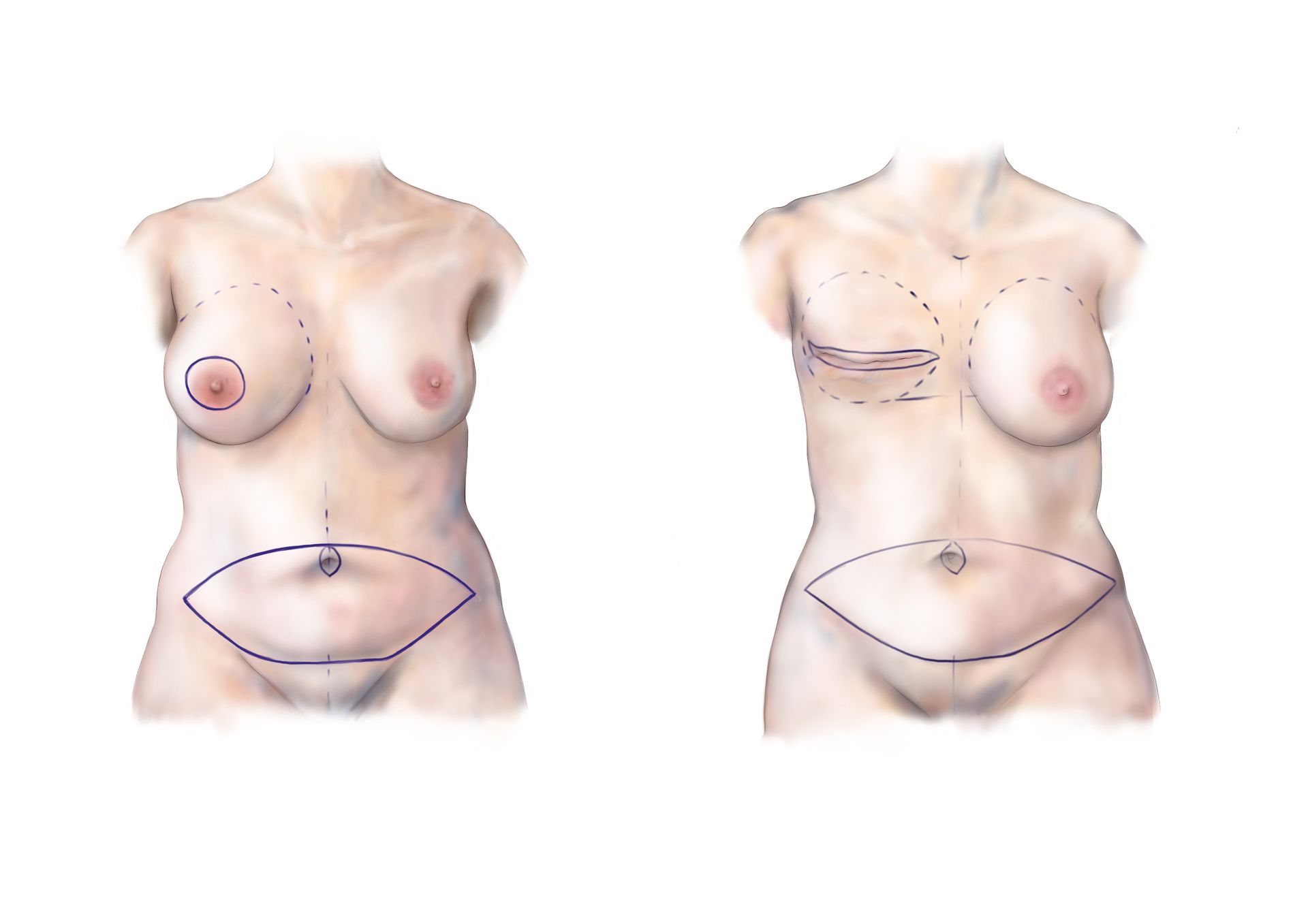
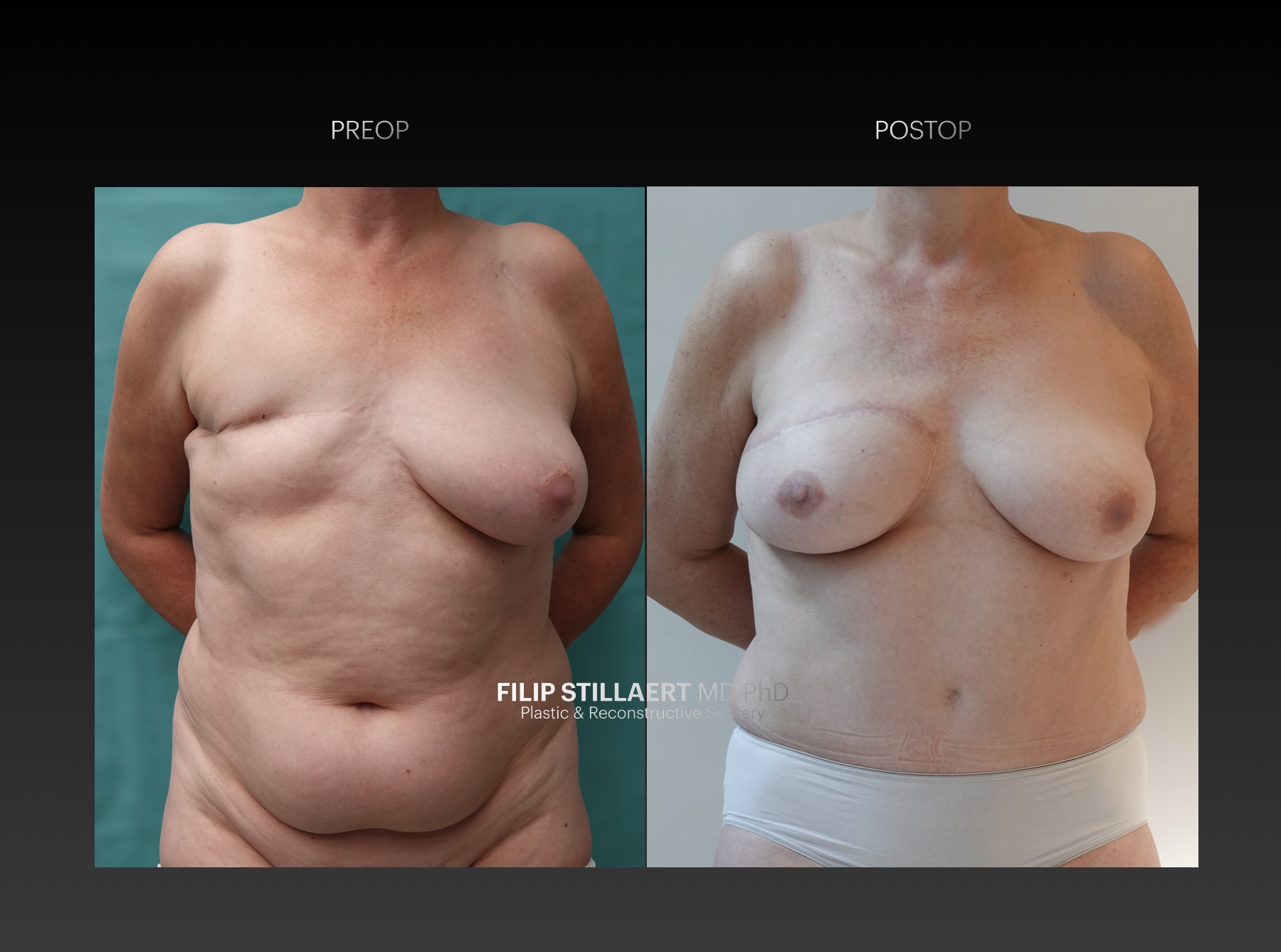
An immediate or primary breast reconstruction is performed simultaneously with the mastectomy. Often, the skin is preserved, and only the "contents" of the breast or the breast glandular tissue needs to be restored. A delayed reconstruction (secondary reconstruction) takes place after a certain period following the mastectomy. In this case, it is often necessary to restore the skin as well.